Learning Objectives
- Identify the axial muscles of the face, head, and neck
- Identify the movement and function of the face, head, and neck muscles
The skeletal muscles are divided into axial (muscles of the trunk and head) and appendicular (muscles of the arms and legs) categories. This system reflects the bones of the skeleton system, which are also arranged in this manner. The axial muscles are grouped based on location, function, or both. Some of the axial muscles may seem to blur the boundaries because they cross over to the appendicular skeleton. The first grouping of the axial muscles you will review includes the muscles of the head and neck, then you will review the muscles of the vertebral column, and finally you will review the oblique and rectus muscles.
Muscles That Create Facial Expression
The origins of the muscles of facial expression are on the surface of the skull (remember, the origin of a muscle does not move). The insertions of these muscles have fibers intertwined with connective tissue and the dermis of the skin. Because the muscles insert in the skin rather than on bone, when they contract, the skin moves to create facial expression (Figure 11.7).

The orbicularis oris is a circular muscle that moves the lips, and the orbicularis oculi is a circular muscle that closes the eye. The occipitofrontalis muscle moves up the scalp and eyebrows. The muscle has a frontal belly and an occipital (near the occipital bone on the posterior part of the skull) belly. In other words, there is a muscle on the forehead (frontalis) and one on the back of the head (occipitalis), but there is no muscle across the top of the head. Instead, the two bellies are connected by a broad tendon called the epicranial aponeurosis, or galea aponeurosis (galea = “apple”). The physicians originally studying human anatomy thought the skull looked like an apple.
The majority of the face is composed of the buccinator muscle, which compresses the cheek. This muscle allows you to whistle, blow, and suck; and it contributes to the action of chewing. There are several small facial muscles, one of which is the corrugator supercilii, which is the prime mover of the eyebrows. Place your finger on your eyebrows at the point of the bridge of the nose. Raise your eyebrows as if you were surprised and lower your eyebrows as if you were frowning. With these movements, you can feel the action of the corrugator supercilli. Additional muscles of facial expression are presented in Figure 11.8.

Muscles That Move the Eyes
The movement of the eyeball is under the control of the extrinsic eye muscles, which originate outside the eye and insert onto the outer surface of the white of the eye. These muscles are located inside the eye socket and cannot be seen on any part of the visible eyeball (Figure 11.9 and Table 11.3). If you have ever been to a doctor who held up a finger and asked you to follow it up, down, and to both sides, he or she is checking to make sure your eye muscles are acting in a coordinated pattern.



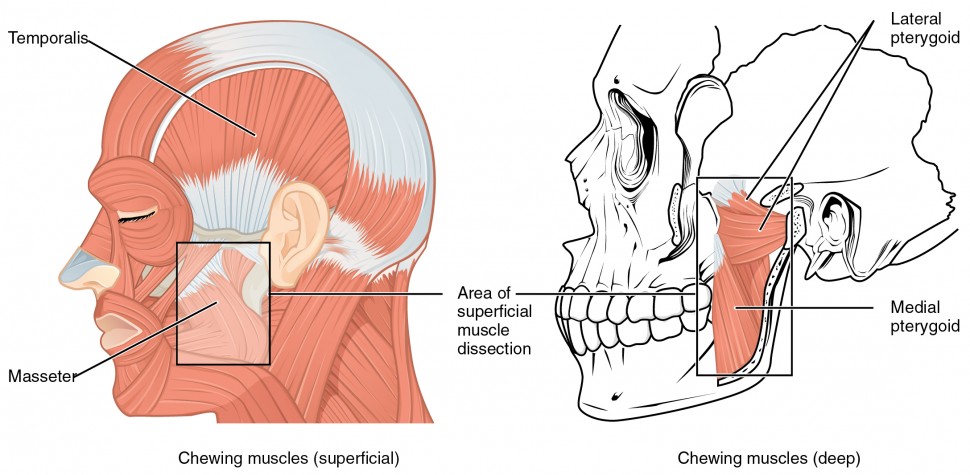
Muscles That Move the Lower Jaw
In anatomical terminology, chewing is called mastication. Muscles involved in chewing must be able to exert enough pressure to bite through and then chew food before it is swallowed (Figure 11.10 and Table 11.4). The masseter muscle is the main muscle used for chewing because it elevates the mandible (lower jaw) to close the mouth, and it is assisted by the temporalis muscle, which retracts the mandible. You can feel the temporalis move by putting your fingers to your temple as you chew.


Muscles That Move the Tongue
Although the tongue is obviously important for tasting food, it is also necessary for mastication, deglutition (swallowing), and speech (Figure 11.11 and Figure 11.12). Because it is so moveable, the tongue facilitates complex speech patterns and sounds.


Tongue muscles can be extrinsic or intrinsic. Extrinsic tongue muscles insert into the tongue from outside origins, and the intrinsic tongue muscles insert into the tongue from origins within it. The extrinsic muscles move the whole tongue in different directions, whereas the intrinsic muscles allow the tongue to change its shape (such as, curling the tongue in a loop or flattening it).
The extrinsic muscles all include the word root glossus (glossus = “tongue”), and the muscle names are derived from where the muscle originates. The genioglossus (genio = “chin”) originates on the mandible and allows the tongue to move downward and forward. The styloglossus originates on the styloid bone, and allows upward and backward motion. The palatoglossus originates on the soft palate to elevate the back of the tongue, and the hyoglossus originates on the hyoid bone to move the tongue downward and flatten it.
Everyday Connections: Anesthesia and the Tongue Muscles
Before surgery, a patient must be made ready for general anesthesia. The normal homeostatic controls of the body are put “on hold” so that the patient can be prepped for surgery. Control of respiration must be switched from the patient’s homeostatic control to the control of the anesthesiologist. The drugs used for anesthesia relax a majority of the body’s muscles.
Among the muscles affected during general anesthesia are those that are necessary for breathing and moving the tongue. Under anesthesia, the tongue can relax and partially or fully block the airway, and the muscles of respiration may not move the diaphragm or chest wall. To avoid possible complications, the safest procedure to use on a patient is called endotracheal intubation. Placing a tube into the trachea allows the doctors to maintain a patient’s (open) airway to the lungs and seal the airway off from the oropharynx. Post-surgery, the anesthesiologist gradually changes the mixture of the gases that keep the patient unconscious, and when the muscles of respiration begin to function, the tube is removed. It still takes about 30 minutes for a patient to wake up, and for breathing muscles to regain control of respiration. After surgery, most people have a sore or scratchy throat for a few days.
Muscles of the Anterior Neck
The muscles of the anterior neck assist in deglutition (swallowing) and speech by controlling the positions of the larynx (voice box), and the hyoid bone, a horseshoe-shaped bone that functions as a solid foundation on which the tongue can move. The muscles of the neck are categorized according to their position relative to the hyoid bone (Figure 11.13). Suprahyoid muscles are superior to it, and the infrahyoid muscles are located inferiorly.

The suprahyoid muscles raise the hyoid bone, the floor of the mouth, and the larynx during deglutition. These include the digastric muscle, which has anterior and posterior bellies that work to elevate the hyoid bone and larynx when one swallows; it also depresses the mandible. The stylohyoid muscle moves the hyoid bone posteriorly, elevating the larynx, and the mylohyoid muscle lifts it and helps press the tongue to the top of the mouth. The geniohyoid depresses the mandible in addition to raising and pulling the hyoid bone anteriorly.
The strap-like infrahyoid muscles generally depress the hyoid bone and control the position of the larynx. The omohyoid muscle, which has superior and inferior bellies, depresses the hyoid bone in conjunction with the sternohyoid and thyrohyoid muscles. The thyrohyoid muscle also elevates the larynx’s thyroid cartilage, whereas the sternothyroid depresses it to create different tones of voice.
Muscles That Move the Head
The head, attached to the top of the vertebral column, is balanced, moved, and rotated by the neck muscles (Table 11.5). When these muscles act unilaterally, the head rotates. When they contract bilaterally, the head flexes or extends. The major muscle that laterally flexes and rotates the head is the sternocleidomastoid. In addition, both muscles working together are the flexors of the head. Place your fingers on both sides of the neck and turn your head to the left and to the right. You will feel the movement originate there. This muscle divides the neck into anterior and posterior triangles when viewed from the side (Figure 11.14).


Muscles of the Posterior Neck and the Back
The posterior muscles of the neck are primarily concerned with head movements, like extension. The back muscles stabilize and move the vertebral column, and are grouped according to the lengths and direction of the fascicles.
The splenius muscles originate at the midline and run laterally and superiorly to their insertions. From the sides and the back of the neck, the splenius capitis inserts onto the head region, and the splenius cervicis extends onto the cervical region. These muscles can extend the head, laterally flex it, and rotate it (Figure 11.15).

The erector spinae group forms the majority of the muscle mass of the back and it is the primary extensor of the vertebral column. It controls flexion, lateral flexion, and rotation of the vertebral column, and maintains the lumbar curve. The erector spinae comprises the iliocostalis (laterally placed) group, the longissimus (intermediately placed) group, and the spinalis (medially placed) group.
The iliocostalis group includes the iliocostalis cervicis, associated with the cervical region; the iliocostalis thoracis, associated with the thoracic region; and the iliocostalis lumborum, associated with the lumbar region. The three muscles of the longissimus group are the longissimus capitis, associated with the head region; the longissimus cervicis, associated with the cervical region; and the longissimus thoracis, associated with the thoracic region. The third group, the spinalis group, comprises the spinalis capitis (head region), the spinalis cervicis (cervical region), and the spinalis thoracis (thoracic region).
The transversospinales muscles run from the transverse processes to the spinous processes of the vertebrae. Similar to the erector spinae muscles, the semispinalis muscles in this group are named for the areas of the body with which they are associated. The semispinalis muscles include the semispinalis capitis, the semispinalis cervicis, and the semispinalis thoracis. The multifidus muscle of the lumbar region helps extend and laterally flex the vertebral column.
Important in the stabilization of the vertebral column is the segmental muscle group, which includes the interspinales and intertransversarii muscles. These muscles bring together the spinous and transverse processes of each consecutive vertebra. Finally, the scalene muscles work together to flex, laterally flex, and rotate the head. They also contribute to deep inhalation. The scalene muscles include the anterior scalene muscle (anterior to the middle scalene), the middle scalene muscle (the longest, intermediate between the anterior and posterior scalenes), and the posterior scalene muscle (the smallest, posterior to the middle scalene).
Candela Citations
- Chapter 11. Authored by: OpenStax College. Provided by: Rice University. Located at: http://cnx.org/contents/14fb4ad7-39a1-4eee-ab6e-3ef2482e3e22@7.1@7.1.. Project: Anatomy & Physiology. License: CC BY: Attribution. License Terms: Download for free at http://cnx.org/content/col11496/latest/.