Describe the structure and function of antibodies
An antibody, also known as an immunoglobulin (Ig), is a protein that is produced by plasma cells after stimulation by an antigen. Antibodies are the functional basis of humoral immunity. Antibodies occur in the blood, in gastric and mucus secretions, and in breast milk. Antibodies in these bodily fluids can bind pathogens and mark them for destruction by phagocytes before they can infect cells.
Learning Objectives
- Describe the structure of antibodies
- Identify the different classes of antibodies
- Describe the function of antibodies
- Describe immunodeficiency and hypersensitivity
Antibody Structure
An antibody molecule is comprised of four polypeptides: two identical heavy chains (large peptide units) that are partially bound to each other in a “Y” formation, which are flanked by two identical light chains (small peptide units), as illustrated in Figure 1. Bonds between the cysteine amino acids in the antibody molecule attach the polypeptides to each other. The areas where the antigen is recognized on the antibody are variable domains and the antibody base is composed of constant domains.

Figure 1. (a) As a germ-line B cell matures, an enzyme called DNA recombinase randomly excises V and J segments from the light chain gene. Splicing at the mRNA level results in further gene rearrangement. As a result, (b) each antibody has a unique variable region capable of binding a different antigen.
In germ-line B cells, the variable region of the light chain gene has 40 variable (V) and five joining (J) segments. An enzyme called DNA recombinase randomly excises most of these segments out of the gene, and splices one V segment to one J segment. During RNA processing, all but one V and J segment are spliced out. Recombination and splicing may result in over 106 possible VJ combinations. As a result, each differentiated B cell in the human body typically has a unique variable chain. The constant domain, which does not bind antibody, is the same for all antibodies.
Similar to TCRs and BCRs, antibody diversity is produced by the mutation and recombination of approximately 300 different gene segments encoding the light and heavy chain variable domains in precursor cells that are destined to become B cells. The variable domains from the heavy and light chains interact to form the binding site through which an antibody can bind a specific epitope on an antigen. The numbers of repeated constant domains in Ig classes are the same for all antibodies corresponding to a specific class. Antibodies are structurally similar to the extracellular component of the BCRs, and B cell maturation to plasma cells can be visualized in simple terms as the cell acquires the ability to secrete the extracellular portion of its BCR in large quantities.
Antibody Classes
Antibodies can be divided into five classes—IgM, IgG, IgA, IgD, IgE—based on their physiochemical, structural, and immunological properties. IgGs, which make up about 80 percent of all antibodies, have heavy chains that consist of one variable domain and three identical constant domains. IgA and IgD also have three constant domains per heavy chain, whereas IgM and IgE each have four constant domains per heavy chain. The variable domain determines binding specificity and the constant domain of the heavy chain determines the immunological mechanism of action of the corresponding antibody class. It is possible for two antibodies to have the same binding specificities but be in different classes and, therefore, to be involved in different functions.
After an adaptive defense is produced against a pathogen, typically plasma cells first secrete IgM into the blood. BCRs on naïve B cells are of the IgM class and occasionally IgD class. IgM molecules make up approximately ten percent of all antibodies. Prior to antibody secretion, plasma cells assemble IgM molecules into pentamers (five individual antibodies) linked by a joining (J) chain, as shown in Figure 2. The pentamer arrangement means that these macromolecules can bind ten identical antigens. However, IgM molecules released early in the adaptive immune response do not bind to antigens as stably as IgGs, which are one of the possible types of antibodies secreted in large quantities upon re-exposure to the same pathogen.
Immunoglobulins have different functions, but all are composed of light and heavy chains that form a Y-shaped structure. Table 1 summarizes the properties of immunoglobulins and illustrates their basic structures.
| Table 1. The Five Immunoglobulin (Ig) Classes | ||
|---|---|---|
| Name | Properties | Structure |
| IgA | Found in mucous, saliva, tears, and breast milk. Protects against pathogens. |  |
| IgD | Part of the B cell receptor. Activates basophils and mast cells. |  |
| IgE | Protects against parasitic worms. Responsible for allergic reactions. | |
| IgG | Secreted by plasma cells in the blood. Able to cross the placenta into the fetus. | |
| IgM | May be attached to the surface of a B cell or secreted into the blood. Responsible for early stages of immunity. |  |
IgAs populate the saliva, tears, breast milk, and mucus secretions of the gastrointestinal, respiratory, and genitourinary tracts. Collectively, these bodily fluids coat and protect the extensive mucosa (4000 square feet in humans). The total number of IgA molecules in these bodily secretions is greater than the number of IgG molecules in the blood serum. A small amount of IgA is also secreted into the serum in monomeric form. Conversely, some IgM is secreted into bodily fluids of the mucosa. Similar to IgM, IgA molecules are secreted as polymeric structures linked with a J chain. However, IgAs are secreted mostly as dimeric molecules, not pentamers.
IgE is present in the serum in small quantities and is best characterized in its role as an allergy mediator. IgD is also present in small quantities. Similar to IgM, BCRs of the IgD class are found on the surface of naïve B cells. This class supports antigen recognition and maturation of B cells to plasma cells.
Antibodies of the Mucosal Immune System
Antibodies synthesized by the mucosal immune system include IgA and IgM. Activated B cells differentiate into mucosal plasma cells that synthesize and secrete dimeric IgA, and to a lesser extent, pentameric IgM. Secreted IgA is abundant in tears, saliva, breast milk, and in secretions of the gastrointestinal and respiratory tracts. Antibody secretion results in a local humoral response at epithelial surfaces and prevents infection of the mucosa by binding and neutralizing pathogens.
Antibody Functions
Differentiated plasma cells are crucial players in the humoral response, and the antibodies they secrete are particularly significant against extracellular pathogens and toxins. Antibodies circulate freely and act independently of plasma cells. Antibodies can be transferred from one individual to another to temporarily protect against infectious disease. For instance, a person who has recently produced a successful immune response against a particular disease agent can donate blood to a nonimmune recipient and confer temporary immunity through antibodies in the donor’s blood serum. This phenomenon is called passive immunity; it also occurs naturally during breastfeeding, which makes breastfed infants highly resistant to infections during the first few months of life.
Antibodies coat extracellular pathogens and neutralize them, as illustrated in Figure 3, by blocking key sites on the pathogen that enhance their infectivity (such as receptors that “dock” pathogens on host cells). Antibody neutralization can prevent pathogens from entering and infecting host cells, as opposed to the CTL-mediated approach of killing cells that are already infected to prevent progression of an established infection. The neutralized antibody-coated pathogens can then be filtered by the spleen and eliminated in urine or feces.
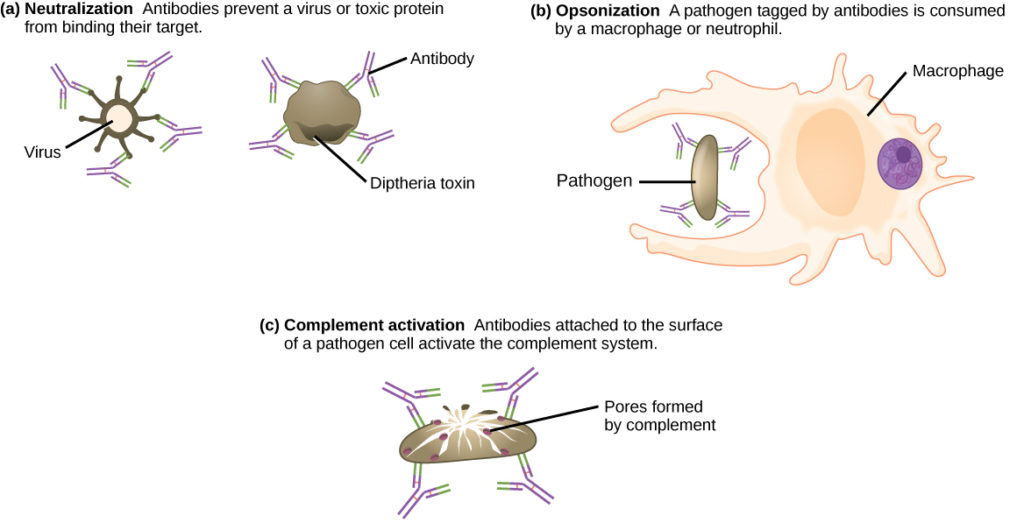
Figure 3. Antibodies may inhibit infection by (a) preventing the antigen from binding its target, (b) tagging a pathogen for destruction by macrophages or neutrophils, or (c) activating the complement cascade.
Antibodies also mark pathogens for destruction by phagocytic cells, such as macrophages or neutrophils, because phagocytic cells are highly attracted to macromolecules complexed with antibodies. Phagocytic enhancement by antibodies is called opsonization. In a process called complement fixation, IgM and IgG in serum bind to antigens and provide docking sites onto which sequential complement proteins can bind. The combination of antibodies and complement enhances opsonization even further and promotes rapid clearing of pathogens.
Affinity, Avidity, and Cross Reactivity
Not all antibodies bind with the same strength, specificity, and stability. In fact, antibodies exhibit different affinities (attraction) depending on the molecular complementarity between antigen and antibody molecules, as illustrated in Figure 4. An antibody with a higher affinity for a particular antigen would bind more strongly and stably, and thus would be expected to present a more challenging defense against the pathogen corresponding to the specific antigen.

Figure 4. (a) Affinity refers to the strength of single interaction between antigen and antibody, while avidity refers to the strength of all interactions combined. (b) An antibody may cross react with different epitopes.
The term avidity describes binding by antibody classes that are secreted as joined, multivalent structures (such as IgM and IgA). Although avidity measures the strength of binding, just as affinity does, the avidity is not simply the sum of the affinities of the antibodies in a multimeric structure. The avidity depends on the number of identical binding sites on the antigen being detected, as well as other physical and chemical factors. Typically, multimeric antibodies, such as pentameric IgM, are classified as having lower affinity than monomeric antibodies, but high avidity. Essentially, the fact that multimeric antibodies can bind many antigens simultaneously balances their slightly lower binding strength for each antibody/antigen interaction.
Antibodies secreted after binding to one epitope on an antigen may exhibit cross reactivity for the same or similar epitopes on different antigens. Because an epitope corresponds to such a small region (the surface area of about four to six amino acids), it is possible for different macromolecules to exhibit the same molecular identities and orientations over short regions. Cross reactivity describes when an antibody binds not to the antigen that elicited its synthesis and secretion, but to a different antigen.
Cross reactivity can be beneficial if an individual develops immunity to several related pathogens despite having only been exposed to or vaccinated against one of them. For instance, antibody cross reactivity may occur against the similar surface structures of various Gram-negative bacteria. Conversely, antibodies raised against pathogenic molecular components that resemble self molecules may incorrectly mark host cells for destruction and cause autoimmune damage. Patients who develop systemic lupus erythematosus (SLE) commonly exhibit antibodies that react with their own DNA. These antibodies may have been initially raised against the nucleic acid of microorganisms but later cross-reacted with self-antigens. This phenomenon is also called molecular mimicry.
Disruptions in the Immune System
Immune disruptions may involve insufficient immune responses or inappropriate immune targets. Immunodeficiency increases an individual’s susceptibility to infections and cancers. Hypersensitivities are misdirected responses either to harmless foreign particles, as in the case of allergies, or to host factors, as in the case of autoimmunity. Reactions to self components may be the result of molecular mimicry.
Immunodeficiency
A functioning immune system is essential for survival, but even the sophisticated cellular and molecular defenses of the mammalian immune response can be defeated by pathogens at virtually every step. In the competition between immune protection and pathogen evasion, pathogens have the advantage of more rapid evolution because of their shorter generation time and other characteristics. For instance, Streptococcus pneumoniae (bacterium that cause pneumonia and meningitis) surrounds itself with a capsule that inhibits phagocytes from engulfing it and displaying antigens to the adaptive immune system. Staphylococcus aureus (bacterium that can cause skin infections, abscesses, and meningitis) synthesizes a toxin called leukocidin that kills phagocytes after they engulf the bacterium. Other pathogens can also hinder the adaptive immune system. HIV infects TH cells via their CD4 surface molecules, gradually depleting the number of TH cells in the body; this inhibits the adaptive immune system’s capacity to generate sufficient responses to infection or tumors. As a result, HIV-infected individuals often suffer from infections that would not cause illness in people with healthy immune systems but which can cause devastating illness to immune-compromised individuals. Maladaptive responses of immune cells and molecules themselves can also disrupt the proper functioning of the entire system, leading to host cell damage that could become fatal.
Failures, insufficiencies, or delays at any level of the immune response can allow pathogens or tumor cells to gain a foothold and replicate or proliferate to high enough levels that the immune system becomes overwhelmed. Immunodeficiency is the failure, insufficiency, or delay in the response of the immune system, which may be acquired or inherited. Immunodeficiency can be acquired as a result of infection with certain pathogens (such as HIV), chemical exposure (including certain medical treatments), malnutrition, or possibly by extreme stress. For instance, radiation exposure can destroy populations of lymphocytes and elevate an individual’s susceptibility to infections and cancer. Dozens of genetic disorders result in immunodeficiencies, including Severe Combined Immunodeficiency (SCID), Bare lymphocyte syndrome, and MHC II deficiencies. Rarely, primary immunodeficiencies that are present from birth may occur. Neutropenia is one form in which the immune system produces a below-average number of neutrophils, the body’s most abundant phagocytes. As a result, bacterial infections may go unrestricted in the blood, causing serious complications.
Hypersensitivities
Maladaptive immune responses toward harmless foreign substances or self antigens that occur after tissue sensitization are termed hypersensitivities. The types of hypersensitivities include immediate, delayed, and autoimmunity. A large proportion of the population is affected by one or more types of hypersensitivity.
Allergies

Figure 5. On first exposure to an allergen, an IgE antibody is synthesized by plasma cells in response to a harmless antigen. The IgE molecules bind to mast cells, and on secondary exposure, the mast cells release histamines and other modulators that affect the symptoms of allergy. (credit: modification of work by NIH)
The immune reaction that results from immediate hypersensitivities in which an antibody-mediated immune response occurs within minutes of exposure to a harmless antigen is called an allergy. In the United States, 20 percent of the population exhibits symptoms of allergy or asthma, whereas 55 percent test positive against one or more allergens. Upon initial exposure to a potential allergen, an allergic individual synthesizes antibodies of the IgE class via the typical process of APCs presenting processed antigen to TH cells that stimulate B cells to produce IgE. This class of antibodies also mediates the immune response to parasitic worms. The constant domain of the IgE molecules interact with mast cells embedded in connective tissues. This process primes, or sensitizes, the tissue. Upon subsequent exposure to the same allergen, IgE molecules on mast cells bind the antigen via their variable domains and stimulate the mast cell to release the modified amino acids histamine and serotonin; these chemical mediators then recruit eosinophils which mediate allergic responses.
Figure 5 shows an example of an allergic response to ragweed pollen. The effects of an allergic reaction range from mild symptoms like sneezing and itchy, watery eyes to more severe or even life-threatening reactions involving intensely itchy welts or hives, airway contraction with severe respiratory distress, and plummeting blood pressure. This extreme reaction is known as anaphylactic shock. If not treated with epinephrine to counter the blood pressure and breathing effects, this condition can be fatal.
Delayed hypersensitivity is a cell-mediated immune response that takes approximately one to two days after secondary exposure for a maximal reaction to be observed. This type of hypersensitivity involves the TH1 cytokine-mediated inflammatory response and may manifest as local tissue lesions or contact dermatitis (rash or skin irritation). Delayed hypersensitivity occurs in some individuals in response to contact with certain types of jewelry or cosmetics. Delayed hypersensitivity facilitates the immune response to poison ivy and is also the reason why the skin test for tuberculosis results in a small region of inflammation on individuals who were previously exposed to Mycobacterium tuberculosis. That is also why cortisone is used to treat such responses: it will inhibit cytokine production.
Autoimmunity

Figure 6. Systemic lupus erythematosus is characterized by autoimmunity to the individual’s own DNA and/or proteins, which leads to varied dysfunction of the organs. (credit: modification of work by Mikael Häggström)
Autoimmunity is a type of hypersensitivity to self antigens that affects approximately five percent of the population. Most types of autoimmunity involve the humoral immune response. Antibodies that inappropriately mark self components as foreign are termed autoantibodies. In patients with the autoimmune disease myasthenia gravis, muscle cell receptors that induce contraction in response to acetylcholine are targeted by antibodies. The result is muscle weakness that may include marked difficultly with fine and/or gross motor functions. In systemic lupus erythematosus, a diffuse autoantibody response to the individual’s own DNA and proteins results in various systemic diseases. As illustrated in Figure 6, systemic lupus erythematosus may affect the heart, joints, lungs, skin, kidneys, central nervous system, or other tissues, causing tissue damage via antibody binding, complement recruitment, lysis, and inflammation.
Autoimmunity can develop with time, and its causes may be rooted in molecular mimicry. Antibodies and TCRs may bind self antigens that are structurally similar to pathogen antigens, which the immune receptors first raised. As an example, infection with Streptococcus pyogenes (bacterium that causes strep throat) may generate antibodies or T cells that react with heart muscle, which has a similar structure to the surface of S. pyogenes. These antibodies can damage heart muscle with autoimmune attacks, leading to rheumatic fever. Insulin-dependent (Type 1) diabetes mellitus arises from a destructive inflammatory TH1 response against insulin-producing cells of the pancreas. Patients with this autoimmunity must be injected with insulin that originates from other sources.
Check Your Understanding
Answer the question(s) below to see how well you understand the topics covered in the previous section. This short quiz does not count toward your grade in the class, and you can retake it an unlimited number of times.
Use this quiz to check your understanding and decide whether to (1) study the previous section further or (2) move on to the next section.
Candela Citations
- Introduction to Antibodies. Provided by: Lumen Learning. License: CC BY: Attribution
- Biology. Provided by: OpenStax CNX. Located at: http://cnx.org/contents/185cbf87-c72e-48f5-b51e-f14f21b5eabd@10.8. License: CC BY: Attribution. License Terms: Download for free at http://cnx.org/contents/185cbf87-c72e-48f5-b51e-f14f21b5eabd@10.8