The Health Belief Model
The Health Belief Model (HBM) was developed in the early 1950s by social scientists at the U.S. Public Health Service in order to understand the failure of people to adopt disease prevention strategies or screening tests for the early detection of disease. Later uses of HBM were for patients’ responses to symptoms and compliance with medical treatments. The HBM suggests that a person’s belief in a personal threat of an illness or disease together with a person’s belief in the effectiveness of the recommended health behavior or action will predict the likelihood the person will adopt the behavior.
The HBM derives from psychological and behavioral theory with the foundation that the two components of health-related behavior are 1) the desire to avoid illness, or conversely get well if already ill; and, 2) the belief that a specific health action will prevent, or cure, illness. Ultimately, an individual’s course of action often depends on the person’s perceptions of the benefits and barriers related to health behavior. There are six constructs of the HBM. The first four constructs were developed as the original tenets of the HBM. The last two were added as research about the HBM evolved.
- Perceived susceptibility – This refers to a person’s subjective perception of the risk of acquiring an illness or disease. There is wide variation in a person’s feelings of personal vulnerability to an illness or disease.
- Perceived severity – This refers to a person’s feelings on the seriousness of contracting an illness or disease (or leaving the illness or disease untreated). There is wide variation in a person’s feelings of severity, and often a person considers the medical consequences (e.g., death, disability) and social consequences (e.g., family life, social relationships) when evaluating the severity.
- Perceived benefits – This refers to a person’s perception of the effectiveness of various actions available to reduce the threat of illness or disease (or to cure illness or disease). The course of action a person takes in preventing (or curing) illness or disease relies on consideration and evaluation of both perceived susceptibility and perceived benefit, such that the person would accept the recommended health action if it was perceived as beneficial.
- Perceived barriers – This refers to a person’s feelings on the obstacles to performing a recommended health action. There is wide variation in a person’s feelings of barriers, or impediments, which lead to a cost/benefit analysis. The person weighs the effectiveness of the actions against the perceptions that it may be expensive, dangerous (e.g., side effects), unpleasant (e.g., painful), time-consuming, or inconvenient.
- Cue to action – This is the stimulus needed to trigger the decision-making process to accept a recommended health action. These cues can be internal (e.g., chest pains, wheezing, etc.) or external (e.g., advice from others, illness of family member, newspaper article, etc.).
- Self-efficacy – This refers to the level of a person’s confidence in his or her ability to successfully perform a behavior. This construct was added to the model most recently in mid-1980. Self-efficacy is a construct in many behavioral theories as it directly relates to whether a person performs the desired behavior.
watch
Limitations of Health Belief Model
There are several limitations of the HBM which limit its utility in public health. Limitations of the model include the following:
- It does not account for a person’s attitudes, beliefs, or other individual determinants that dictate a person’s acceptance of a health behavior.
- It does not take into account behaviors that are habitual and thus may inform the decision-making process to accept a recommended action (e.g., smoking).
- It does not take into account behaviors that are performed for non-health related reasons such as social acceptability.
- It does not account for environmental or economic factors that may prohibit or promote the recommended action.
- It assumes that everyone has access to equal amounts of information on the illness or disease.
- It assumes that cues to action are widely prevalent in encouraging people to act and that “health” actions are the main goal in the decision-making process.
The HBM is more descriptive than explanatory, and does not suggest a strategy for changing health-related actions. In preventive health behaviors, early studies showed that perceived susceptibility, benefits, and barriers were consistently associated with the desired health behavior; perceived severity was less often associated with the desired health behavior. The individual constructs are useful, depending on the health outcome of interest, but for the most effective use of the model it should be integrated with other models that account for the environmental context and suggest strategies for change.
The Social Cognitive Theory
Social Cognitive Theory (SCT) started as the Social Learning Theory (SLT) in the 1960s by Albert Bandura. It developed into the SCT in 1986 and posits that learning occurs in a social context with a dynamic and reciprocal interaction of the person, environment, and behavior. The unique feature of SCT is the emphasis on social influence and its emphasis on external and internal social reinforcement. SCT considers the unique way in which individuals acquire and maintain behavior, while also considering the social environment in which individuals perform the behavior. The theory takes into account a person’s past experiences, which factor into whether behavioral action will occur. These past experiences influences reinforcements, expectations, and expectancies, all of which shape whether a person will engage in a specific behavior and the reasons why a person engages in that behavior.
Many theories of behavior used in health promotion do not consider maintenance of behavior, but rather focus on initiating behavior. This is unfortunate as maintenance of behavior, and not just initiation of behavior, is the true goal in public health. The goal of SCT is to explain how people regulate their behavior through control and reinforcement to achieve goal-directed behavior that can be maintained over time. The first five constructs were developed as part of the SLT; the construct of self-efficacy was added when the theory evolved into SCT.
- Reciprocal Determinism – This is the central concept of SCT. This refers to the dynamic and reciprocal interaction of person (individual with a set of learned experiences), environment (external social context), and behavior (responses to stimuli to achieve goals).
- Behavioral Capability – This refers to a person’s actual ability to perform a behavior through essential knowledge and skills. In order to successfully perform a behavior, a person must know what to do and how to do it. People learn from the consequences of their behavior, which also affects the environment in which they live.
- Observational Learning – This asserts that people can witness and observe a behavior conducted by others, and then reproduce those actions. This is often exhibited through “modeling” of behaviors. If individuals see successful demonstration of a behavior, they can also complete the behavior successfully.
- Reinforcements – This refers to the internal or external responses to a person’s behavior that affect the likelihood of continuing or discontinuing the behavior. Reinforcements can be self-initiated or in the environment, and reinforcements can be positive or negative. This is the construct of SCT that most closely ties to the reciprocal relationship between behavior and environment.
- Expectations – This refers to the anticipated consequences of a person’s behavior. Outcome expectations can be health-related or not health-related. People anticipate the consequences of their actions before engaging in the behavior, and these anticipated consequences can influence successful completion of the behavior. Expectations derive largely from previous experience. While expectancies also derive from previous experience, expectancies focus on the value that is placed on the outcome and are subjective to the individual.
- Self-efficacy – This refers to the level of a person’s confidence in his or her ability to successfully perform a behavior. Self-efficacy is unique to SCT although other theories have added this construct at later dates, such as the Theory of Planned Behavior. Self-efficacy is influenced by a person’s specific capabilities and other individual factors, as well as by environmental factors (barriers and facilitators).
watch
Limitation of Social Cognitive Theory
There are several limitations of SCT, which should be considered when using this theory in public health. Limitations of the model include the following:
- The theory assumes that changes in the environment will automatically lead to changes in the person, when this may not always be true.
- The theory is loosely organized, based solely on the dynamic interplay between person, behavior, and environment. It is unclear the extent to which each of these factors into actual behavior and if one is more influential than another.
- The theory heavily focuses on processes of learning and in doing so disregards biological and hormonal predispositions that may influence behaviors, regardless of past experience and expectations.
- The theory does not focus on emotion or motivation, other than through reference to past experience. There is minimal attention on these factors.
- The theory can be broad-reaching, so can be difficult to operationalize in entirety.
Social Cognitive Theory considers many levels of the social ecological model in addressing behavior change of individuals. SCT has been widely used in health promotion given the emphasis on the individual and the environment, the latter of which has become a major point of focus in recent years for health promotion activities. As with other theories, applicability of all the constructs of SCT to one public health problem may be difficult especially in developing focused public health programs.
The Theory of Planned Behavior
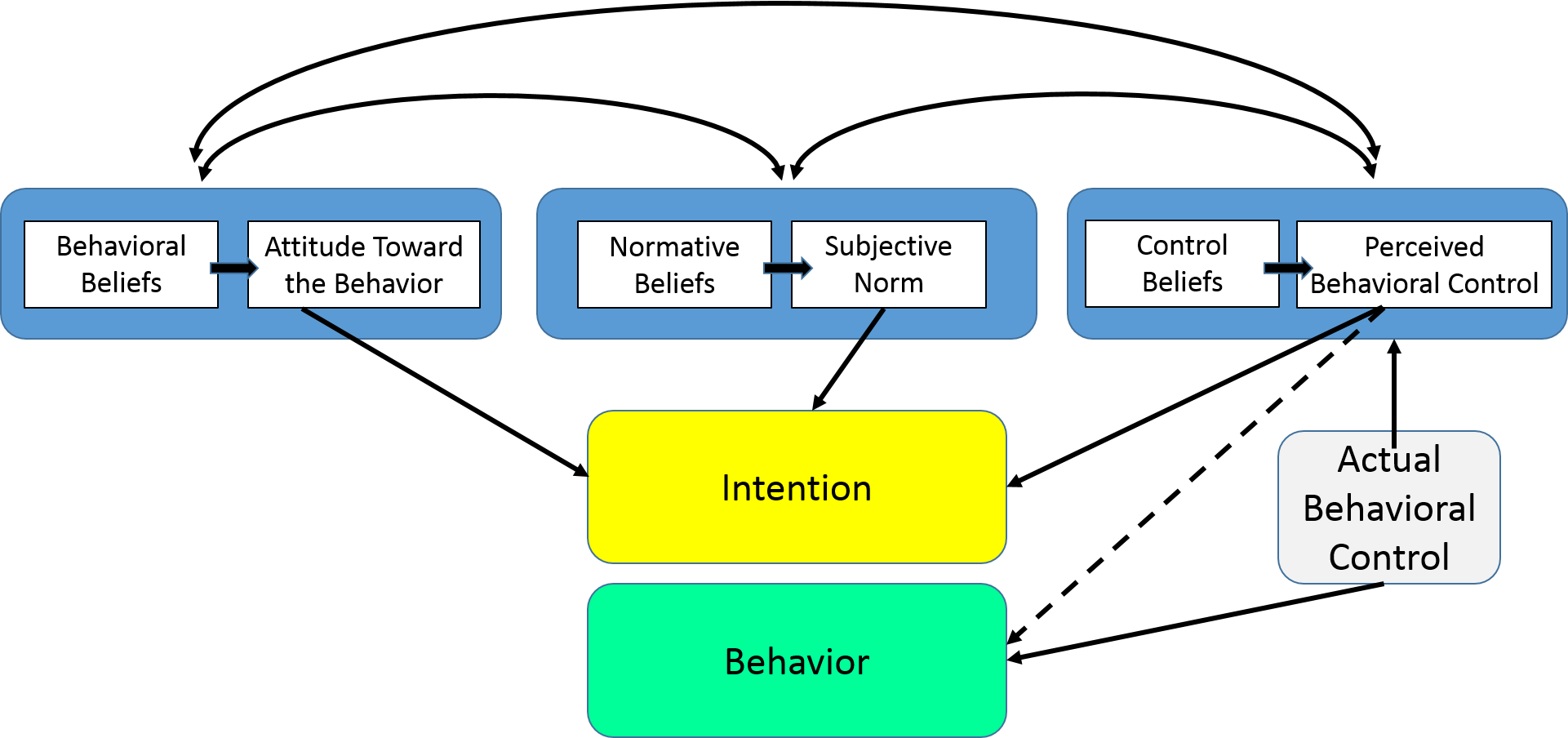
The Theory of Planned Behavior (TPB) started as the Theory of Reasoned Action in 1980 to predict an individual’s intention to engage in a behavior at a specific time and place. The theory was intended to explain all behaviors over which people have the ability to exert self-control. The key component to this model is behavioral intent; behavioral intentions are influenced by the attitude about the likelihood that the behavior will have the expected outcome and the subjective evaluation of the risks and benefits of that outcome.
The TPB has been used successfully to predict and explain a wide range of health behaviors and intentions including smoking, drinking, health services utilization, breastfeeding, and substance use, among others. The TPB states that behavioral achievement depends on both motivation (intention) and ability (behavioral control). It distinguishes between three types of beliefs – behavioral, normative, and control. The TPB is comprised of six constructs that collectively represent a person’s actual control over the behavior.
- Attitudes – This refers to the degree to which a person has a favorable or unfavorable evaluation of the behavior of interest. It entails a consideration of the outcomes of performing the behavior.
- Behavioral intention – This refers to the motivational factors that influence a given behavior where the stronger the intention to perform the behavior, the more likely the behavior will be performed.
- Subjective norms – This refers to the belief about whether most people approve or disapprove of the behavior. It relates to a person’s beliefs about whether peers and people of importance to the person think he or she should engage in the behavior.
- Social norms – This refers to the customary codes of behavior in a group or people or larger cultural context. Social norms are considered normative, or standard, in a group of people.
- Perceived power – This refers to the perceived presence of factors that may facilitate or impede performance of a behavior. Perceived power contributes to a person’s perceived behavioral control over each of those factors.
- Perceived behavioral control – This refers to a person’s perception of the ease or difficulty of performing the behavior of interest. Perceived behavioral control varies across situations and actions, which results in a person having varying perceptions of behavioral control depending on the situation. This construct of the theory was added later, and created the shift from the Theory of Reasoned Action to the Theory of Planned Behavior.
Limitations of the Theory of Planned Behavior
There are several limitations of the TPB, which include the following:
- It assumes the person has acquired the opportunities and resources to be successful in performing the desired behavior, regardless of the intention.
- It does not account for other variables that factor into behavioral intention and motivation, such as fear, threat, mood, or past experience.
- While it does consider normative influences, it still does not take into account environmental or economic factors that may influence a person’s intention to perform a behavior.
- It assumes that behavior is the result of a linear decision-making process, and does not consider that it can change over time.
- While the added construct of perceived behavioral control was an important addition to the theory, it doesn’t say anything about actual control over behavior.
- The time frame between “intent” and “behavioral action” is not addressed by the theory.
The TPB has shown more utility in public health than the Health Belief Model, but it is still limiting in its inability to consider environmental and economic influences. Over the past several years, researchers have used some constructs of the TPB and added other components from behavioral theory to make it a more integrated model. This has been in response to some of the limitations of the TPB in addressing public health problems.
watch
Candela Citations
- The Theory Of Planned Behavior, The Social Cognitive Theory, The Health Belief Model. Authored by: Wayne W. LaMorte, MD, PhD, MPH . Provided by: Boston University School of Public Health . Located at: https://sphweb.bumc.bu.edu/otlt/mph-modules/sb/behavioralchangetheories/BehavioralChangeTheories3.html. License: All Rights Reserved
